
TURKISH FORUM 2014 YILINDA ALANLARINDA IZ BIRAKMIS EN BASARILI MESLEK INSANLARINI ONURLANDIRIYOR
Yazan Prof. Dr. Gul Celkan –
Ocak 23, 2015
TURKISH FORUM 2014 YILINDA ALANLARINDA IZ BIRAKMIS EN BASARILI MESLEK INSANLARINI ONURLANDIRIYOR
Turkish Forum, Amerika Birleşik Devletleri’nde yaşayan Türklerin, Türk asıllı Amerikalıların ve Amerikalı Türk dostlarının 1993 yılında temelini attığı ve şu anda dünyanın beş kıtasına dağılmış, birçok ülkede yerel çalışma grupları ile örgütlenmiş Türkiye dışında yaşayan Türk’lerin büyük bölümüne ulaşan gönüllü çalışan bağımsız bir sivil toplum örgütüdür. Turkish Forum, kar amacı gütmeyen, döner sermayesi olmayan, kurulduğundan bu yana Türkiye ve Türk toplumunun hizmetinde olmuş, nice başarılı projelerin ve kampanyaların gerçekleşmesinde basrolü oynamış, moral ve heyecanı yüksek, toplumun maddi ve manevi desteği ile ayakta duran ABD’de kayıtlı Türkiye Cumhuriyeti tarafından da tanınan bir sivil toplum örgütüdür.
Turkish Forum’un misyonu Türkiye Cumhuriyetinin dünyaya tanıtılmasında öncü rol oynamak olduğu kadar tarihe ışık tutmak ve kitleleri bilgilendirmektir. Turkish Forum dünyayı saran haber ağı ve pek çok ülkedeki alt örgütleri sayesinde, Türkiye ile ilgili haberlerden dünyaya dağılmış Türkler ve dostlarını haberdar edip, yerel yönetimlerde daha aktif hale gelmelerini amaçlar. Bulunduğu bölge ve ilgili konularda araştırmalar yaparak, fikirler geliştirir. Türk toplulukları arasındaki iletişimi güçlendirerek farklı ülkelerde dağınık vaziyette bulunan Türk’lerin ve dostlarının örgütlenerek güçlenebilmesini hedefler.
Bu misyonunuz çerçevesinde, Turkish Forum ve Dünya Turkleri Birligi olarak her yil kendi alanlarinda yaptiklari çalişmalarla, topluma katkilariyla, yapitlariyla ön plana cikan meslek insanlarinin ödüllendirilmeleri ve basarialrini kamuoyu ile paylasmak amaciyla bir proje baslatmistik ve Turkish Forum Danisma Kurulu Uyelerinin katkilariyla farkli alanlarda calismalariyla on plana cikan meslek insanlarimizi saptadik.
2014 yilinda ilk kez yaptigimiz bu proje onumuzdeki yillarda da devam edecek ve her yil yine bu donemlerde bir onceki yilda basarilariyla iz birakmis meslek insanlarini onurlandirip kamuoyu ile paylasacagiz.
Yapilan calismalar sonucunda bu yil kendi dallarinda/alanlarinda basarili calismalara imza atan ve icinde bulunduklari topluma katki koyan isimler sirasiyla Sefika Guney, Yard.Doc. Dr.Mustafa Aksoy, Doc.Dr.Mehmet Toy, Melissa Azize Gokmogol, Dr. Fusun Cetin Cuhadaroglu, Prof.Dr. Selcuk Kuyucak, Dilek Ergul, Ergün Kirlikovalı, Dr. Baran Sümer ve Dr. Hakan Gürsu.
Kendi alanlarinda on plana cikan ve ozelde icinde bulunduklari topluma ve genelde Turkiye’nin adinin farkli platformlarda anilmasina katki koyan bu isimlerin onerilme surecinde ve degerlendirilmesinde gorev alan tum Turkish Forum Danisma Kurulu uyelerimize ve Yonetim Kuruluna tesekkur ediyor, sonuclari tum Turk Dunyasi ile paylasabilmenin hakli gururunu yasarken, kendilerini bir kez daha kutluyorum.
Saygilarimla,
Dr. Kayaalp Buyukataman
CEO Yon. Kurulu Baskani
Turkish Forum – Dunya Turkleri Birligi
- SEFIKA GUNEY

Bugun 13 yasinda olan Sefika, 11 yasindayken kaleme aldigi Melis adli romaniyla Turkiye’nin en genc yazari unvanina sahip. Canim Dostumla Birlikte ise Sefika’nin ilk oyku kitabi. Dokuz oykuden olusan bu kitabinda aile ve arkadaslik iliskileri, hayvanlarla kurulan dostluklar, yeni baslangiclarin getirdigi heyecanlar ve insanlik hallerine iliskin pek cok ayrinti 13 yasindaki Sefika’nin naïf anlatimiyla aktariliyor. Kullandigi dil ise gunumuz yazarlarina tas cikaracak nitelikte. Sefika’nin herkese bir mesaji var: “Bol okumali gunler dilerim.”
Sefika Wechsler Cocuklar icin Zeka Olcegi sonucuna gore 135 puanla Ustun Zekali bir cocuk oldugu yonunde sertifika sahibidir.
Sefika’yi kendi anlatimiyla taniyalim: “Ben aslında çok da şanlı bir çocuk değilim. Neden derseniz ben sadece okuma ve yazma konusundaki yeteneklerimi aile desteği ile sürdürmeye çalışıyorum. Ama resim yeteneğim ,zekam günden güne köreliyor. Muğla’da üstün zekalı çocuklar için ayrı bir eğitim almıyorum. Yasal hakkım olduğu halde alamıyorum.
Üstüne üstlük bir de TÜYAP da Ahmet Ümit, Ayşe Kulin gibi yazarlarla aynı gün imza vereceğim. Ezilmekten korkuyorum. Bu yaşlarda benim kaygılarım bu olmamalıydı. Elbette çok erken yaşlarda kitap yazmam iyi oldu,elbette ki kitabımın Türkiye’nin en büyük yayınevinin basması iyi oldu( Ayşe Kulin Güneşe Dön Yüzünü adlı eserini bastırmak için 20 yıl yayınevi aramis) ama
bazen ticari kaygılar bir çocuk kalbinin kaldıramıyacağı yükler bindiriyor.”
Kitaplarinin tanitimi amaciyla bu kucuk yasina ragmen Istanbul’da, Samsun’da ve baska kentlerde Kitap Fuarlarina katilip kitaplarini imzalayan, soylesilere katilan kucuk yazarimizi kutluyor, calismalarinda ustun basarilar diliyoruz.
- DOC. DR.MUSTAFA AKSOY


Tarihin Sessiz Dili Damgalar kitabinin yazari Yard. Doc. Dr. Mustafa Aksoy, 1959 Kadirli dogumlu. Firat Univeristesi’nden 1982 yilinda kayit oldugu zaman Anropoloji olarak bilinen bolumden 1986 yilinda Sosyoloji lisans derecesi ile mezun olduktan sonra Istanbul Universitesinde Yuksek Lisans ve Doktora calismalarini tamamlamistir. Calismalarini uygulamali sosyolojiye olan ilgisi yuzunden bu yonde yogunlastirmistir. Saha çalışması yaptığı ülkeler:
Tamamen kendi olanaklarıyla, Türkiye -özellikle Doğu ve Güneydoğu Anadolu’da-, İran, Azerbaycan, Ukrayna, Türkmenistan, Özbekistan, Kazakistan, Kırgızistan, Altay, Hakasya ve Tuva’da, UKİD (Uluslararası Kalkınma Yardımları ve İşbirliği Derneği) katkılarıyla da Moldavya, Romanya ve Kosova’da saha araştırmaları yaptı. Halen saha çalışmalarına devam etmektedir.
Dr. Aksoy’un 18 yillik emeginin urunu olan Tarihin Sessiz Dili Damgalar ile Turkish Forum’un “2014 yili Basarili Meslek Insanlarini Onurlandirma” projesine onerilmis ve komisyonun hayranligini kazanmistir. Aksoy, kitabini hazirlama asamasinda zorluklarla karsilastigini ve tüm olumsuzluklara karşın kendi deyisiyle bu çalışma, bir sevdanın sonucu olarak ortaya çıkmıştır. Başka bir deyişle kitap âdeta “damga”ların izinde geçirilmiş yılların ürünüdür. Yorucu, büyük bir emek ve sabır isteyen on altı yıllık bir zaman dilimini kapsamış olsa da her araştırma sahasında ayrı bir mutluluk tadılmış, bu kitabın meydana gelebilmesi adına sevinç ve üzüntü duygularının birlikte var olduğu zorlu bir süreç yaşanmıştır.
Araştırmalarım sırasında “damgaları kimlerin ve niçin yaptığı, damgaların kaynağının ne olduğu” sorularına cevap bulmaya çalışan yazar, “Bu damgaları niçin yapıyorsunuz?” sorusuna on altı yıl boyunca aldığım cevaplar, “Atamdan böyle gördüm, anamdan böyle gördüm, bunlar bizim geleneğimiz, tarihten beri bunları hep yapıyoruz” şeklinde olmuştur.
Tarihin Sessiz Dili Damgalar 14 ülkede saha araştırmaları yapılarak, 18 yılda hazırlanan kitaptir; en çok kullanılan 208 damganın çizimi yapılarak, damgalar dizini oluşturulmuş ve 14 ülkeden 579 fotoğraf kullanılmıştır.
Eser, halı-kilim ve diğer dokumalarla, at koşumları, kaya resimleri, mezar taşları, evlerin dış cepheleri, sokak işaretleriyle, otobüs duraklarında karşılaştığımız veya arkeolojik ve etnografik eserlerden günümüze kadar gelmiş olan maddi kültür unsurlarındaki “işaretler” ile “damgalar” üzerinde, 14 ülkede saha çalışmaları yapılarak tespit edilmiş verilere dayanılarak hazırlanmıştır.
Bahsedilen maddi kültür unsurlarındaki “şekil” ve “damgalar” yorumlanarak farklı bir kültür tarihi yazılmıştır. Ayrıca entografik eserlerin görülenden farklı boyutları olduğu, bunların en “otantik tarihi belgeler” olarak kabul edilmeleri gerektiği belirtilmiştir.
Aksoy, “damgalar”ın tarihin bilinen kadim dönemlerinden günümüze kadar geldikleri ve taşıdıkları anlamlarla tarihe şahitlik ettiklerine dikkat çekerek, etnografik eserlere farklı bakış açısı ve bir “kültür teorisi” önermiştir.
Dr. Aksoy’u; onemli bir basvuru kaynagi olacagina inandigimiz bu cok basarili eseri kaleme aldigi icin kutluyoruz. Ancak Aksoy, henuz arastirmasinin tamamlanmadigini, amacinin ilk firsatta Yakut’lardan Alaskaya uzanan genis bir cografyada devam ettirmek oldugunu belirtmistir. Kendisine calismalarinda Turkish Forum olarak ustun basarilar diliyoruz.
- DR. MEHMET TOY

Turk-Amerikan Dernekleri Asamblesi Baskanligina yeni secilen Dr. Toy, goreve geldigi gunden itibaren yeni bir vizyon ve misyon getirerek catisi altinda topladigi dernekler ile son derece uyumlu ve birlik icin calisan bir baskan olma ozellligini tasimaktadir,
Ayrica Ermeni ve diger Turk aleyhtari propagandalara karsi kuvvetli cevaplar vermekte- son TUSIAD ve Bogazici Universitesinin tek tarafli konferansina karsi yaptigi atilim herkesin takdirini kazanmisti. Goreve geldigi gunden beri bir seri seminarlar duzenlenmesine onculuk ederek her ay Amerikanin cesitli yerlerinde farkli konularda iki ayri konferans duzenlenmesine onculuk ederek dernekleri bir araya getirme ve aydinlatma calismalarina devam etmektedir.
New Jersey, New York ve Pennsylvania eyaletlerinde yasayan Turk toplumunun ABD senatosunda ve kongresinde, New Jersey senatosunda ve kongresinde, sozde Ermeni soykirimi konusunda aleyhimize cikabilecek tasarilara karsi aktivitelerini organize etmek ve yonlendirmekfedir.
Ayrica ATAA Mutevelli Heyeti uyeligi ve Yatirim Komitesi baskanligi. ITU-MD USA Yonetim Kurulu Uyeligi de vardir.
Sadece ATAA Baskani olarak degil kendi alaninda da basarili calismalara imza atmistir. Bilgisayar aglari konusunda ki calismalariyla uluslararasi alanda taninan bir bilim adami, muhendis ve idarecidir. Yayinlamis oldugu bes kitap, bir video ve sayisiz makaleleriyle ifade ettigi calismalarinin bir kismi uluslarasi standardlar haline donusturulmus ve yillardir endustri de kullanilmaktadir. Yaptigi calismalardan dolayi cesitli firmalardan ve uluslararasi kuruluslardan oduller almistir.
Almis Oldugu Oduller ve Burslar; Inventor Awards (Mucit Odulleri), Comcast
Exceptional Contribution Awards, AT&T Bell Labs ve Lucent Technologies
PACE Leadership Award, IEEE(Institute of Electrical and Electronics Engineers)-USA , AT&T Federal Systems Silver Award , MEB Yurt Disi Doktora Bursu , KOC Bursu ve TUBITAK Bursu olarak sayilabilir.
Sayin Toy’u hem Turk Amerikan toplumuna yapmakta oldugu katkilarindan hem de yenilikci bilimsel calismalarindan dolayi kutluyor ve calismalarinda Turkish Forum olarak ustun basarilar diliyoruz.
- MELISSA AZIZE GOKMOGOL

Melissa Gökmoğol 1992 senesinden beri Amerika’da gönüllü olarak politikada çalışmalar yapmaktadır. Gerek başkanlık seçimleri, gerek yerel seçimlerde değişik alanlarda görevlerde bulunmuştur. 2008 Başkanlık seçimleri kampanyasında bölge yöneticiliği ve 2012 senesinde United States Congressman’nın kampanyasında stratejik araştırma görevlisi olarak görev yapmıştır. 2014 senesinde ise, Indiana eyaletinin tek Türk Kadın parti delegesi olarak seçilmiştir.
Başkanlık seçimlerine ve partinin tüzüklerine imza atan parti delegeleri olarak Indiana eyaletini temsil eden tek ve ilk Türk kadınıdır. United States Congressman’ı olan Todd Rokita’nın kampanyasında 2012 senesinde olduğu gibi 2014’de de başarılı kampanya hizmetlerine devam etmiştir. Ayrıca Indiana’daki 2014 yerel seçimlerinde hakim adayı ve Indiana eyaletinin Congressman’ı olmak için aday olan başka bir kişinin kampanyasının yönetim kurulunda görev almıştır. Melissa Gökmoğol Purdue Üniversitesi Siyasal Bilgiler Bölümünü onur derecesi ile bitirip, The George Washington Üniversite’sinde Politika Yönetimi üzerine yüksek lisans yapmaktadır.
Yaptığı bütün çalışmalar ile Türk insanını ve Türk kadınını başarı ile Amerikan siyasetinde tanıtıyor olması ve Indiana eyaletinin tek ve ilk Türk Kadın parti delegesi olmasıdır.
Melissa Gökmoğol Amerika’da politika alanında başarılı olması ile birlikte, iş hayatında da 10 milyon dolardan fazla değeri olan bir şirketi ortaya çıkaran başarılı bir Türk iş kadınıdır.
Melissa Gokmogol’u politika ve is yasami konularinda Turk kadinin adini duyurdugu ve basarili calismalara imza attigi icin kutluyor ve gelecekteki calismalarinda da Turkish Forum olarak ustun basarilar diliyoruz.
- DR. SELCUK KUYUCAK

Kanada’da bulunan McGill’den mezun olan ve calismalarina 1990 yilindan beri CANMET Mobile Foundry Laboratory, Ottawa, Ontario’da devam eden Dr. Kuyucak, Metalurji Malzeme Bilim Dalinda yapmis oldugu calismalarla CANMET den odul kazanmistir. Celik Dokum, ostenitik mangan celiklerinin islemi, oksit takviyeli celiklerin gelistirilmesi konularinda yapmis oldugu basarili calismalarin sonucu olarak mesleki literature dunyada “KUYUCAK METODU” olarak bilinen bir yontem kazandirmistir.
Turk bilim adamalrinin dunyanin neresinde olursa olsun bilime yaptiklari katkilar ulkemiz acisindan da onem tasimaktadir. Kendi adiyla anilan bir yontemi dunya bilim literaturune kazandirmis olmasindan dolayi Turkish Forum olarak kutluyor ve basarili calismalarinin devamini diliyoruz.
- Dr. FUSUN CETIN CUHADAROGLU

Amerikan Çocuk ve Ergen Psikiyatrisi Akademisi tarafından verilen “Ülkü Ülgür Uluslararası Bilim Adamı Ödülü” nün ilk sahibi olan Hacettepe Üniversitesi’nden Prof. Dr. Füsun Çetin Çuhadaroğlu Dr. Ulku Ulgur’un sadece kendiis degil alanda calisan pek cok bilim insani icin bir model olusturdugunu ve bu yuzden de boyle bir odulun cok anlamli oldugunu soylemistir.
Hacettepe Üniversitesi Çocuk ve Ergen Ruh Sağlığı ve Hastalıkları Anabilim Dalı Başkanlığı Öğretim Üyesi Prof. Dr. Füsun Çetin Çuhadaroğlu American Academy of Child and Adolescent Psychiatry (Amerikan Çocuk ve Ergen Psikiyatrisi Akademisi) tarafından “Çocuk psikiyatrisinde örnek alınacak uluslararası bir lider” olarak ” Ülkü Ülgür International Scholar Award” (Uluslararası Bilim Adamı) ödülüne layık görülmustur.
Akademinin ilk uluslararası ödülü olan “Ülkü Ülgür Uluslararası Bilim Adamı” ödülüne layık görülen Dr. Çuhadaroğlu, Türkiye’de Çocuk ve Ergen Psikiyatrisinin ayrı bir tıp dalı olarak kabul edilmesi ve gelişmesine katkıda bulundu. Yüzden fazla yayını ve on sekiz kitap bölümü bulunan Prof. Dr. Çuhadaroğlu ulusal ve uluslararası araştırma kuruluşları tarafından desteklenen projeleri yürüttü ve çeşitli ödüller aldı. Türkiye Çocuk ve Genç Psikiyatrisi Derneği’nin bir meslek kuruluşu olarak kurulup gelişmesi ve kurumsallaşmasına önemli katkıları oldu ve 10 yıl başkanlığını yaptı. Çocuk ve Ergen Psikiyatrisi alanında ulusal ve
uluslararası birçok bilimsel etkinlik ve kongreye imzasını atmış olan Prof. Dr. Çuhadaroğlu halen Avrupa Çocuk ve Ergen Psikiyatrisi Derneği Yönetim Kurulu Üyeliğini sürdürüyor. Çuhadaroğlu, Uluslararası Çocuk ve Ergen Psikiyatrisi ve İlişkili Meslekler Birliği Genel Sekreteri ve Uluslararası Ergen Psikiyatrisi ve Psikolojisi Derneği Başkan Yardımcılığı görevlerini de yürütüyor.
Turkish Forum olarak Sn. Cuhadaroglu’nin uluslarasi arenada da taninan basarili calismalarinin devamini diliyor ve kutluyoruz.
- DILEK ERGUL
.

2014 yilinda sosyal sorumluluk projesi kapsaminda onurlandirilmaya aday gosterilen Dilek Ergul, Atlantik’I kizlar icin gececek. İzmirli amatör bir denizci olan Dilek Ergul, uzun yıllar satış üzerine çalıştı. Ancak işlerine ara verdi ve yelkenliyle 14 aylık bir seyahate çıktı. Şu sıralar Kanarya Adaları’nda dalgalarla sağanak yağmurla boğuşan Ergül, hayali olan Atlantik Okyanusu’nu geçmeyi planlıyor. Üstelik bu yolculuğun bir de amacı var: 10 kız öğrencinin 10 yıl boyunca okumasını sağlamak.
8 Haziran 2014’te İstanbul Avcılar ‘WIM Marina’dan yola çıkan Ergul, bugüne kadar dört ülke, 37 liman şehri ve yedi kara şehrine uğradı. 3.700 deniz mili (6.840 km) yol yaptı.
Bu seyahatini faydalı bir yönde kullanma isteğiyle Darüşşafaka Cemiyeti ile çalışmayı tercih etmesinin nedeni hem okulda verilen eğitimin kalitesi, hem yüzde 100 burs sağlamaları hem de uzun soluklu evlatlarımızın yanında olmalarıni kendisi için harika bir fırsat olarak gormektedir. Böylece ulaşabileceği çocukların geleceklerinden daha emin olabileceğini düşündü. Bu konuda Darüşşafaka Cemiyeti’nden dostları da destek verince ortaya ‘Rota Atlantik Fonu’ çıktı. 10 kız çocuğumuzu 10 yıl okutabilmek amaçlı olarak 1 milyon TL toplamak hedefiyle ROTA ATLANTIK, yelkenler fora diyerek yola cikti.
Dilek Ergul’u hem Turk kadininin neler basarabilcegini gostermesi, hem bayragimizi denizlerde dalgalandirmasi hemde cok guzel bir amac ugruna bu zorlu yolculugu goze aldigi icin kutluyor, basari ile rotasini tamamlamasini diliiyoruz.
8. ERGÜN KIRLIKOVALI

ATAA eski baskani, TF Danisma ve Yonetim Kurullari uyesi, FTAA eski Baskan Yardimcisi olan Ergün Kirlikovalı, yıllardır Türk-Amerikan toplumuna yaptığı hizmetleri ile herkesin takdirini toplamasına ek olarak başarılı bir bilim adamı ve iş adamıdır. Ergün Kirlikovalı’nın asıl büyük hizmeti hiç durmak bilmeden büyük bir enerji ile mücadele ettiği sözde Ermeni soykırımı meselesidir. Yazdığı yazıları çeşitli medya kuruluşları ve Türksih Forum da da yayınlanmasının yanısıra katıldığı ulusal ve uluslararası konferanslarda Türk tezini belgeleriyle savunmuş bir sosyal tarihçi kimliğide taşımaktadır. En son katılmış olduğu ve Boğaziçi Üniversitesi tarafından düzenlenen konferansta yaptığı konuşma da bunun en güzel kanıtıdır.
Sn. Kirlikovalı’nın belkide bu son konferansta söylediği ve belleklerden uzun zaman silinmeyeck olan sözü, “ Tarih ne çağımız politikalarının kölesi ne de birbiriyle yarışan anıların emrinde olmamalıdır.”
Turkish Forum Danışma Kurulu ve Yönetim Kurulu üyeleri oybirliği ile Sn. Kirlikovalı’yı üstün vasıflarıyla başarılı bir sosyal tarihçi olarak 2014 yılının başarılı meslek insanları arasında anılmasına karar vermiştir, Kendisini kutluyor ve başarılı çalışmalarının devamını diliyoruz.
- DR. BARAN SÜMER

Amerika Birleşik Devletleri Texas Üniversitesi KBB Bölümünde çalışmalarını yürüten Dr. Baran Sümer, ÖncoNano Medicine’in kurucuları olan ekibiyle birlikte 6 milyon dolarlık Product Development Grant alarak kanser hastalarının ameliyatları sırasında doktorların tümörü görmelerine olanak sağlayan ve tümörü bütünüyle temizleyip çıkarmalarını sağlayan nano teknolojiye dayanan floresan sondalar geliştirmişlerdir.
Dr. Baran Sümer, 2014 yılı Cancer Prevention & Research Institute of Texas (CPRIT) ödülüne “Onco Nano Medicine: Transforming Cancer Surgery by Tumor Illumination”başlıklı çalışması ile layık görülmüştür.
Turkish Forum – Dünya Türkleri Birliği Danışma Kurulumuuzn önerisi ve Yönetim kurulunun oy blrliği ile aldığı kararla Dr. Baran Sümer’İ Tip Dünyasına ve özellikle kanser hastalarının tedavisine çok büyük katkı koyacak olan bu çalışması ve üstün başarısından dolayı kutluyor ve başarılı çalışmalarının devamını diliyoruz.
- DR. HAKAN GÜRSU

Üniversite sanayi işbirliği çerçevesinde adına kayıtlı Endüstriyel ürün tescili olan Dr. Hakan Gürsu, Orta Doğu Teknik Üniversitesinde çalışmalarını sürdürmektedir.
Dr. Hakan Gürsu sayesinde Türkiye için süper bir şey oldu: dünyanın en özgür zekalarının katıldığı bir yarışmada birinci seçildi.
Bu öyle bir yarışma ki para ödülü bile vermiyorlar. Çünkü hayallere para biçmiyorlar. O yarışmada insanlar birbirleriyle değil, birbirlerinin hayalleriyle yarışıyor. Aklına esenlerle… Uykusunu kaçıranlarla… Düşünde gördükleriyle ve düşünü gerçekleştirenlerle…
Bu yıl 100’un üzerinde milletten katılımın olduğu yarışmada “düş birincisi” ODTÜ Öğretim Üyesi Dr. Hakan Gürsu… Gürsu önce bir tekne düşledi. Öyle bir tekne ki yakıtı olmadan da gitsin. Yelkeni olsun ama rüzgar esmediğinde bile yüzsün. Ve “Volitan” böylece hayalken gerçek oldu.
“Volitan” Latince “hızlı yol alan” demek. Bir de Akdeniz sahillerinde görülen bir uçarbalığın adı… Bu balığın çok saygı duyulacak bir performansı var. 200 metre kadar suyun üzerinde gidiyor. Balığı da, kelimenin anlamını da çok sevdiğini belirten Gürsu, “Xmr21″ gibi bir isim yerine “Volitan” ismine karar kıldıklarını söylüyor.
“Tasarım Oscari” kazanan Dr. Hakan Gürsu’yu hayallerinin projesini gerçekleştirip Türkiye’mize birincilik ödülünü kazandırdığı için Turkish Forum ve Dünya Türkleri Birliği olarak kutluyor, yeni projelerinde üstün başarılar diliyoruz.
- ETİKETLER
- KAYAALP BUYUKATAMAN
- Turkish Forum











 HALK SAĞLIĞINDA İZ BIRAKANLAR
HALK SAĞLIĞINDA İZ BIRAKANLAR



 Yine nedendir diye sormayın (bana göre karıncaları çeken bir kimyasal madde var olmalı) karıncalar bu sümükleri yiyor ve solucanın serkaryaları tarafından enfekte oluyorlar. Genelde gerek salyangoz gerekse karıncalar çimlerin diplerinde inekler tarafından ezilmeden ve yenmeden dolaşıyorlar.
Yine nedendir diye sormayın (bana göre karıncaları çeken bir kimyasal madde var olmalı) karıncalar bu sümükleri yiyor ve solucanın serkaryaları tarafından enfekte oluyorlar. Genelde gerek salyangoz gerekse karıncalar çimlerin diplerinde inekler tarafından ezilmeden ve yenmeden dolaşıyorlar. İşte burada olağan dışı birsey oluyor: Salyangozun sümüğünü yiyen karıncalara geçen serkaryaların çoğunluğu karıncaların karınlarının altında kist halinde duruyor. Birkaç serkarya ise metaserkarya haline geçip ezofaguz (yutma borusu) altındaki karıncaların nöronal ganglionlarına geçip karıncanın davranışını kontrol altına alıyor. Normalde ineklerden kaçan karıncalara bir şeyler oluyor. Normalde sağlıklı karıncalar güneş batıp hava soğumaya başlayınca yuvalarına dönmeye başlıyor. Metaserkaryanın kontrolündeki karıncalar ise gidip çimlerin en taze ve yeşillerinin üstünde çimleri ısırıp sabaha dek bekliyorlar. Eğer inekler gelip çimleri ve onları da yemezse sabah havanın ısınmasıyla normal yaşamlarına dönüyorlar. Taa ki akşama dek.
İşte burada olağan dışı birsey oluyor: Salyangozun sümüğünü yiyen karıncalara geçen serkaryaların çoğunluğu karıncaların karınlarının altında kist halinde duruyor. Birkaç serkarya ise metaserkarya haline geçip ezofaguz (yutma borusu) altındaki karıncaların nöronal ganglionlarına geçip karıncanın davranışını kontrol altına alıyor. Normalde ineklerden kaçan karıncalara bir şeyler oluyor. Normalde sağlıklı karıncalar güneş batıp hava soğumaya başlayınca yuvalarına dönmeye başlıyor. Metaserkaryanın kontrolündeki karıncalar ise gidip çimlerin en taze ve yeşillerinin üstünde çimleri ısırıp sabaha dek bekliyorlar. Eğer inekler gelip çimleri ve onları da yemezse sabah havanın ısınmasıyla normal yaşamlarına dönüyorlar. Taa ki akşama dek.


 Tahtakurusu
Tahtakurusu Sonradan anlaşılmış ki bu bir evrim sonucu kazanılmış üstünlük değil, bir enfeksiyon hastalığı. Bu hastalığın etmeni de Wolbachia pipientis. Bu bakteri zorunlu bir hücre içi parazit ve birçok böcek türünün yumurtalık ve testislerine yerleşiyor.
Sonradan anlaşılmış ki bu bir evrim sonucu kazanılmış üstünlük değil, bir enfeksiyon hastalığı. Bu hastalığın etmeni de Wolbachia pipientis. Bu bakteri zorunlu bir hücre içi parazit ve birçok böcek türünün yumurtalık ve testislerine yerleşiyor.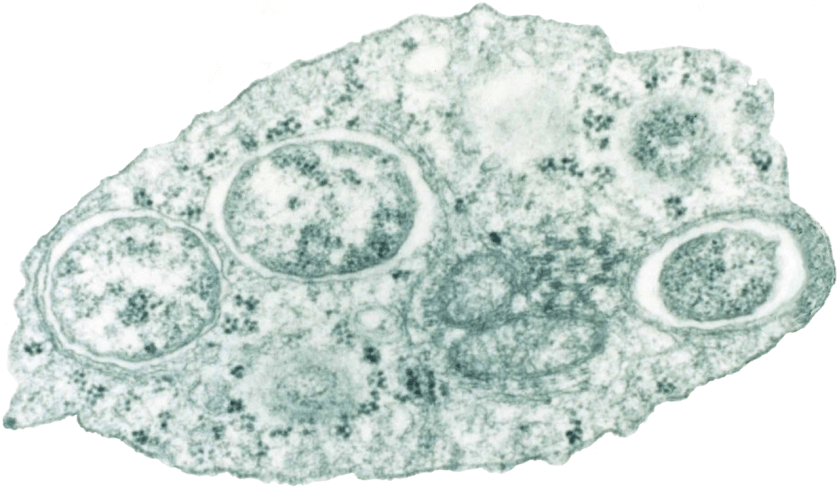








 Yıldızlı Gökyüzü Van Gogh
Yıldızlı Gökyüzü Van Gogh








, oversaw Cyberknife treatments for patient Stephen Wiley.")



 Andrew Holder
Andrew Holder
You must be logged in to post a comment.